
This is the first of a series of 5 blog posts following my participation in the Running Repairs course hosted by The Running Physio (Tom Goom). The information below is a mix of my own reading and the information gleaned from his course (which I highly recommend!)
Proximal hamstring tendinopathy (PHT)
This is one close to my heart, as I am currently suffering from a very annoying proximal hamstring injury. I now know that Tom also spent time away from running with this injury and so I was all ears to hear how he was able to manage it in both himself and patients.
What is it?
PHT presents as a deep buttock pain often localised around ischial tuberosity (bony bit). it can occur in any of the hamstring tendons, although most commonly in biceps femoris and semimembranosus.
A tendinopathy appears to occur on a continuum (Cook JL, Purdam CR 2008, see figure below). From a non inflammatory initial thickening all the way along to a degenerative tendon with areas of disorganised and even dead cells. Excessive load is the main culprit to either progress the tendon along the continuum or elevate it back to a normal, pain free tendon.
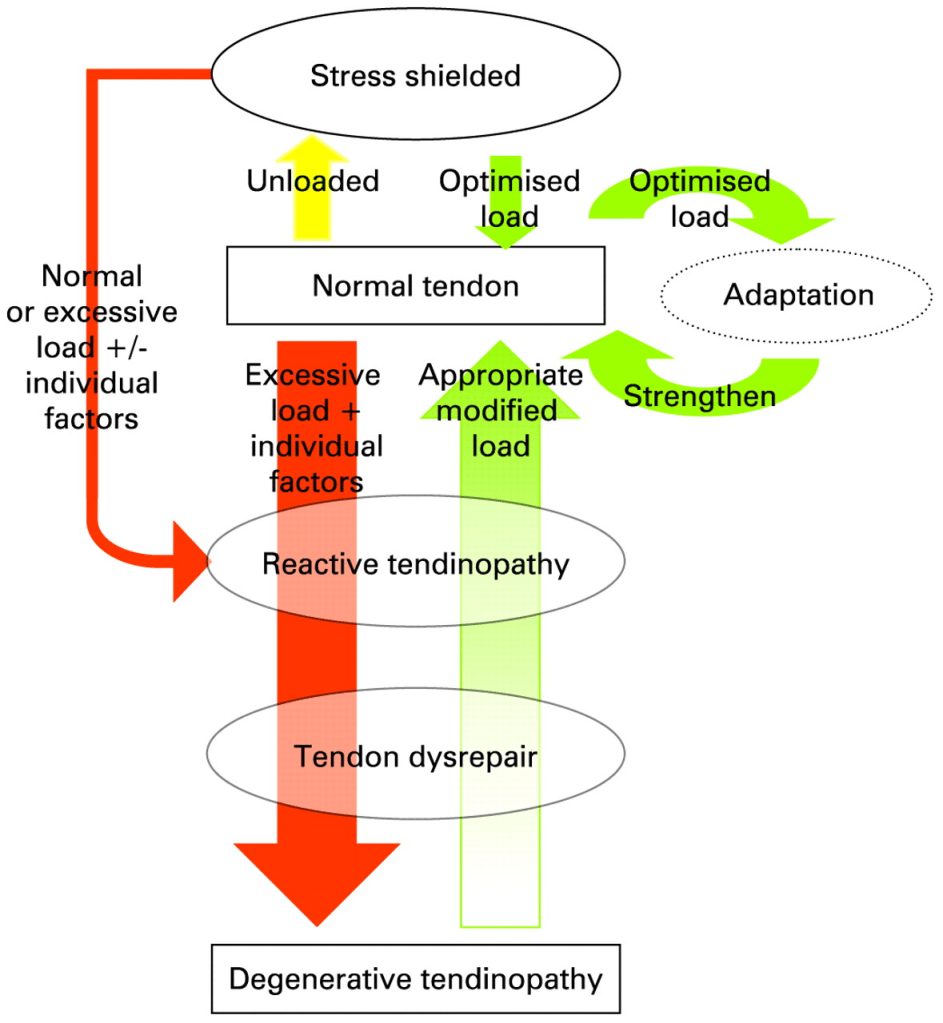
Image taken from Cook JL, Purdam CR 2008. See Reference list below.
Cause –
PHT is a really common condition amongst runners and athletes in both sagittal plane and change of direction sports (Goom et al, 2016).
It is also considered an insertional tendinopathy which changes the way you manage a tendon problem (more on this later).
There are of course Intrinsic factors that contribute to the onset of pathology which Tom’s paper covers (age, BMI, metabolic issues), however I am only focussing on the specific extrinsic factors.
Key aggravating factors in the literature – hip flexion and adduction compress tendon, high loads/ stress and minimal recovery time.
For me – Running (especially uphill and don’t even mention sprinting), sitting for long periods, deadlifts, squats, cycling for long periods, rowing.
Key learning point – The hamstring reaches peek force during running while at late swing phase, as the muscle works eccentrically to slow the leg down and get it ready for impact.
What’s really interesting about this pathology is the nature and timing of pain. This is relatively common knowledge in the physio world but actually very strange and frustrating to feel as someone experiencing it.
Tendons warm up –
Tendon pain often gets better with exercise, this is because the tendon has warmed up and is doing its job. However, once you have finished your workout and the tendon ‘cools down’ there is often a delayed pain response that comes with it.
This is a sign that you’ve ‘overdone it’ and the tendon hasn’t coped with the load you put through it during that workout. This pain can last 24-72 hours and can really put a dent in your motivation to keep training.
Just when you think your tendon problem has disappeared and you’re running pretty much pain free, if you’ve done too much too soon, later on that day, or even the next morning, the tendon has cooled down and will almost definitely kick off a huge pain response to that earlier activity. This makes treatment extremely difficult and requires patience for all parties in involved.
My understanding on how to treat PHT has also developed as a direct result of this experience.
When you first learn about tendon problems as a physio (or as a student) you are taught that the tendon is weak, and therefore needs to be strengthened in order to help resolve the pain. Unfortunately this simply doesn’t work (at least in the initial acute stage) for proximal, or insertional type injuries, often loading them too aggressively will irritate them for days at a time.
Key treatment takeaways –
Stage 1 Early management – Settle symptoms down
Figure out exactly what aggravates your tendon – as described earlier this is commonly cause by hip flexion (especially past 80 degrees, direct contact and pressure too, so raise your office chair or add a cushion!). For me, rolling up a towel or even a jacket and placing it under my thighs really helps – remember you’re offloading the sitting bones.
Deep squats, deadlifts, RDLS, deep leg press can all really aggravate. They’re all asking the hamstring to work too hard EG – running (especially uphill) asks the hamstrings to work eccentrically to slow the leg at terminal swing phase.
During this period, little and often movement is best, avoiding long periods of sitting – probably best to avoid running altogether (especially uphill) unless you can find a distance that doesn’t trigger your pain – remember tendons have a delayed pain onset. You’ll often have to wait a few hours, or even the next day before knowing if you’ve set it off again.
Some exercises that have been helping me in the early painful stage –
Swimming – remember to keep fit and active even if your pain is stopping your normal exercise routine. I’ve used a buoy between my legs to stop myself from kicking in the water as even this can aggravate my symptoms.
Check out my Instagram post here for a few basic hamstring and lower limb exercises to start you off, which shouldn’t aggravate your symptoms.
Mid range hamstring isometrics – these are really to try and settle your symptoms and get some force running through the muscle. Isometrics are the weakest and least force producing contractions you can do.
Glute bridge (lots of variations on this). Double leg, single leg, hamstring bridges. Experiment with what works for you, and where you feel the exercise.
Squat – against the wall or a ball. Avoiding the forward lean in a squat has really helped reduce my symptoms.
Backwards walking – When I have aggravated my symptoms, I actually find that backwards walking is less irritating than walking itself. There is also some small studies suggesting it can help increase hamstring flexibility (CHET R. WHITLEY and JANET S. DUFEK, 2009).
Stage 2 – Return to activity, How much, how often, how intense?
Once pain has settled and you can load through your tendon with these exercises, you might be tempted to trial running again (the fun bit).
I’d say this stage has been the hardest for me, and often with patients I treat. Mainly because of how delayed symptoms normally are, figuring out exactly how much your tendon can manage without flaring can be a mystery. Also because I am generally fit enough to run harder and for longer than my tendon wants, it’s very easy to overdo it.
so remember, run slower than you think, run on the flat and stop sooner rather than later. If you can figure out that your tendon can manage a 3km run at 7 minute per kilometre pace – you suddenly have a baseline to build from. If you come home and you’ve flared the pain up for more than 24 hours, it’s back to the drawing board. Maybe a 2km run will work?
Stage 2-3 Increasing hip flexion –
This is where you can start incorporating those more common and higher load exercises into your routine
Example A) Straight leg deadlift can be an effective way of targeting your hamstrings. I would suggest starting with a low, manageable weight, partial repetitions and ensuring the pain during exercise stays below a <4/10.
Example B) Bodyweight full range of movement squat – heels elevated to reach low if preferred. I like this to start really strengthening the whole lower body – you can trial this exercise, and if the hamstring tolerates it, slowly start adding load as able.
Overall the proximal hamstring tendinopathy is a real pain to both diagnose and treat, but once figured out, you should be able to reduce those aggravating factors and return to the activities (albeit slowly) you enjoy.
I will save the mid-late stage rehab for another blog/ time.
If you made it this far, thanks for reading my first ever blog post! let me know what you thought on my Instagram, twitter etc.
BW,
Elliot.
Future blog posts/ learning points from the course coming up:
Training load vs capacity
Osteoarthritis not linked to running
Can we analyse someone’s gait? and how can we change it?
References –
Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. 2009 Jun;43(6):409-16. doi: 10.1136/bjsm.2008.051193. Epub 2008 Sep 23. PMID: 18812414.
Goom TS, Malliaras P, Reiman MP, Purdam CR. Proximal Hamstring Tendinopathy: Clinical Aspects of Assessment and Management. J Orthop Sports Phys Ther. 2016 Jun;46(6):483-93. doi: 10.2519/jospt.2016.5986. Epub 2016 Apr 15. PMID: 27084841.
Effects of Backward Walking on Hamstring Flexibility and Low Back Range of Motion 2009 (CHET R. WHITLEY*1 and JANET S. DUFEK).
